Discover how the latest HHS rule on information blocking could impact your healthcare practice and Medicare payments. The new rule aims to address the barriers that prevent the secure exchange of electronic health information, ultimately enhancing patient access to their own health data.
By understanding the intricacies of this rule, healthcare professionals can proactively adapt their practices to ensure compliance, avoid potential penalties, and navigate any legal challenges that may arise.
Introduction
On June 24, 2024, the Department of Health and Human Services (HHS) released a groundbreaking final rule that could have significant implications for healthcare providers across the country. This new regulation, aimed at curbing information blocking practices as defined under the 21st Century Cures Act, establishes a stringent framework for penalizing providers found guilty of these practices. With the rule set to take effect soon, healthcare providers need to act quickly to ensure compliance and avoid potentially severe penalties.
What is Information Blocking?
Information blocking involves practices that interfere with the access, exchange, or use of electronic health information (EHI) and can hinder the seamless flow of information critical for patient care. This new rule targets such practices, ensuring that healthcare providers promote interoperability and share information as required.
Key Details of the New Rule
Implementation Date:
The rule will be effective 30 days after its publication in the Federal Register.
Authority and Purpose:
This rule exercises the Secretary’s authority under the 21st Century Cures Act (Cures Act) to establish disincentives for health care providers who engage in information blocking. Information blocking involves practices that providers knew were unreasonable and likely to interfere with access, exchange, or use of EHI.
Disincentives Outlined
Medicare Promoting Interoperability Program
Eligible Hospitals
A reduction in payment by three-quarters of the applicable percentage increase in the market basket update if the hospital fails to demonstrate meaningful EHR use.
Critical Access Hospitals (CAH)
Reduced payment to 100% of reasonable costs from 101% if they fail to meet meaningful EHR use requirements..
Merit-based Incentive Payment System (MIPS)
Eligible Clinicians and Group Practices
A zero score in the Promoting Interoperability performance category for those found guilty of information blocking.
Accountable Care Organization (ACO) – Medicare Shared Savings Program:
ACOs and Participants
Potential denial of participation for one year and other mitigating actions for those found guilty of information blocking.
Implications for Healthcare Providers
Increased Scrutiny:
Healthcare providers should prepare for heightened investigations and monitoring by the OIG regarding their information-sharing practices.
Financial Impact:
The penalties could result in substantial financial losses, particularly for providers who heavily rely on Medicare reimbursements.
Reputational Risk:
Public reporting of violations may damage the reputation of providers found guilty of information blocking.
Compliance Programs
Providers must strengthen their compliance programs to prevent information blocking practices.
Technology Assessment:
Providers should assess their health IT systems and practices to identify and address potential information blocking issues.
Documentation:
Maintaining thorough documentation of information-sharing practices will be crucial in defending against investigations.
Education and Training:
Comprehensive staff training is essential to ensure all team members understand the prohibitions and consequences of information blocking.
Practical Takeaways
This final rule marks a significant step in HHS’s efforts to enforce information blocking prohibitions and promote interoperability in the healthcare system. Healthcare providers, executives, and compliance professionals should:
- Carefully review the rule’s provisions.
- Take proactive steps to ensure compliance.
- Stay informed about OIG’s investigative priorities and any further guidance from HHS.
Complementary Rules
HHS rule complements the OIG’s final rule from June 2023, which established penalties for other actors in the information blocking sphere, including health IT developers, health information exchanges, and health information networks. Violations by these entities can result in civil monetary penalties of up to $1 million per violation.
Potential Legal Challenges
In light of the Supreme Court’s decision in Loper Bright Enterprises v. Raimondo, which ended Chevron deference to federal agencies, there may be opportunities to challenge this final rule. Healthcare providers interested in exploring legal challenges should consult with legal counsel to discuss potential strategies and collective actions.
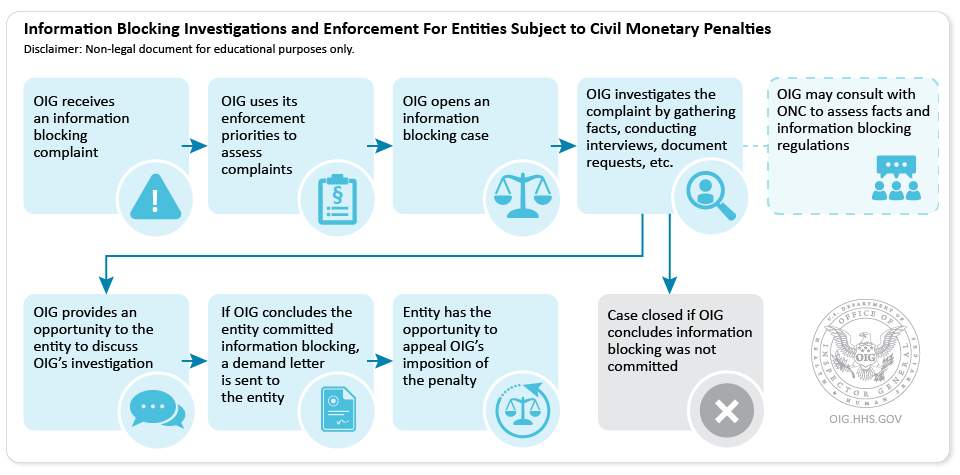
Information Blocking Investigations and Enforcement For Entities Subject to Civil Monetary Penalties
- OIG receives an information blocking complaint
- OIG uses its enforcement priorities to assess complaints
- OIG opens an information blocking case
- OIG investigates the complaint by gathering facts, conducting interviews, document requests, etc.
- OIG may consult with ONC to assess facts and information blocking regulations
- Case closed if OIG concludes information blocking was not committed
- OIG provides an opportunity to the entity to discuss OIG’s investigation
- If OIG concludes the entity committed information blocking, a demand letter is sent to the entity
- Entity has the opportunity to appeal OIG’s imposition of the penalty
Enforcement Priorities
OIG expects that it will receive more information blocking complaints than it can investigate. To triage allegations and allocate resources, OIG will use the following priorities to select cases for investigation:
- Resulted in, is causing, or had the potential to cause patient harm
- Significantly impacted a provider’s ability to care for patients
- Was of long duration
- Caused financial loss to Federal health care programs, or other government or private entities
- Was performed with actual knowledge
For more detail on these priorities and OIG’s approach to enforcing information blocking penalties, please see the rule
Conclusion
The new HHS rule is a pivotal measure in enhancing interoperability and ensuring seamless information sharing in the healthcare system. Providers must adapt quickly, bolster their compliance efforts, and remain vigilant to navigate this evolving regulatory landscape effectively. Failure to comply could result in significant financial and reputational damage, making immediate action essential for all healthcare providers.
FAQs
What is the effective date of the new HHS rule on information blocking?
The rule will take effect 30 days after its publication in the Federal Register.
What penalties are outlined for hospitals under the new rule?
Eligible hospitals may face a reduction in payment by three-quarters of the applicable percentage increase in the market basket update if they fail to demonstrate meaningful EHR use.
How will the rule impact Critical Access Hospitals (CAH)?
CAHs will see a reduced payment to 100% of reasonable costs from 101% if they fail to meet meaningful EHR use requirements.
What are the consequences for MIPS eligible clinicians found guilty of information blocking?
Clinicians or group practices will receive a zero score in the Promoting Interoperability performance category.
How will the rule affect Accountable Care Organizations (ACO)?
ACOs or their participants found guilty of information blocking may face denial of participation for one year and other mitigating actions.
What should healthcare providers do to comply with the new rule?
Providers should strengthen compliance programs, conduct comprehensive staff training, assess health IT systems, and maintain thorough documentation of information-sharing practices.
