2021 CAQH INDEX®
The CAQH Index benchmarks adoption, volume, cost savings opportunities and spend for transactions along the administrative workflow.
The CAQH Index benchmarks adoption, volume, cost savings opportunities and spend for transactions along the administrative workflow. The following metrics help measure progress towards an automated workflow. By tracking progress, the industry can more easily identify barriers that may be delaying automation and administrative simplification and focus efforts on them.
ADMINISTRATIVE WORKFLOW
While COVID-19 touched all healthcare professionals, the pandemic impacted the medical and dental administrative workflows differently.
The following touches on MEDICAL and DENTAL.
Utilization
Policies developed by federal and state entities to curb the spread of COVID-19 resulted in lower utilization for both industries as people delayed, or went without, medical care. In general, lower utilization led to lower transaction volumes. Smaller dental practices were hit particularly hard by lower utilization as many offices were forced to close for several months or close permanently.
Spend
Although electronic adoption and volume increased for both industries, the spend associated with conducting administrative transactions varied. While the dental industry saw a drop in spend, the medical industry experienced an increase in spend as it dealt with more complicated factors related to COVID-19
Automation
As remote work increased, many medical and dental staff became more reliant on the use of electronic transactions to conduct business. Staff no longer had access to resources used to conduct manual transactions. Because of this, both industries saw an increase in electronic adoption.
Telemedicine
For the medical industry, the loss in volume was counterbalanced by the increase in telemedicine. Telemedicine expanded access to care while reducing exposure to the virus for staff and patients. Health plans and providers worked together to understand and confirm new requirements and varying codes around telemedicine which often resulted in costly and timely phone calls and manual work. And while manual volume dropped, manual transactions became more expensive, increasing overall spend and the
cost savings opportunity.
While manual volume dropped, manual transactions became more expensive, increasing overall spend and the cost savings opportunity.
While manual volume dropped, manual transactions became more expensive, increasing overall spend and the cost savings opportunity.
Tweet
VOLUME
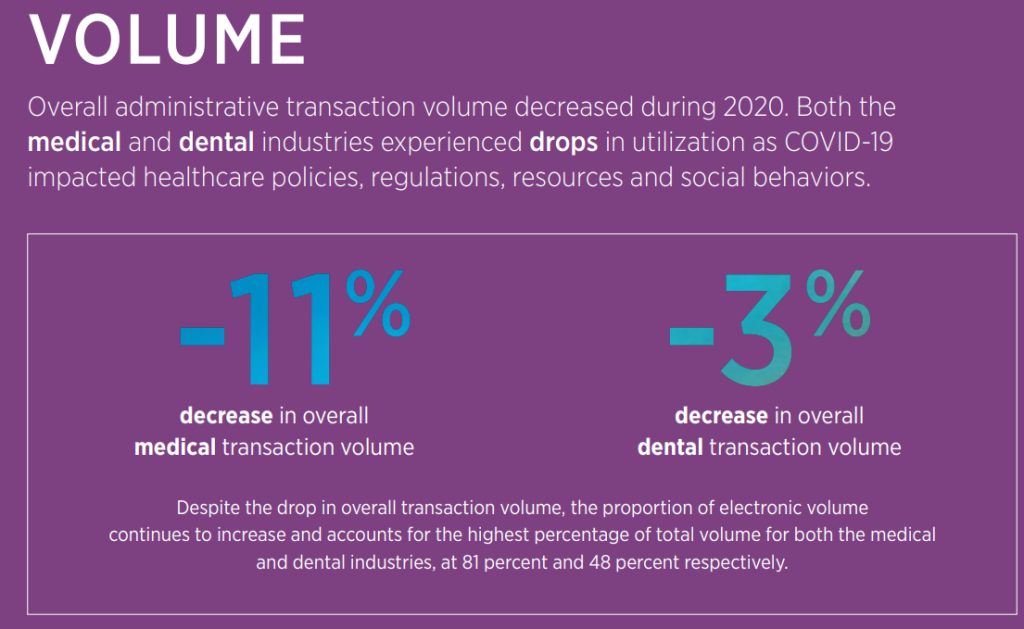
Overall administrative transaction volume decreased during 2020. Both the
medical and dental industries experienced drops in utilization as COVID-19
impacted healthcare policies, regulations, resources and social behaviors.
SPEND
Despite the decrease in overall medical transaction volume and growth in electronic adoption, total annual medical spend increased (12%) as manual transactions required more intensive intervention from providers to ensure that newly implemented requirements and codes were executed correctly and that patient medical records were current and accurate. Conversely, dental spending decreased due to lower utilization often resulting in office closures.

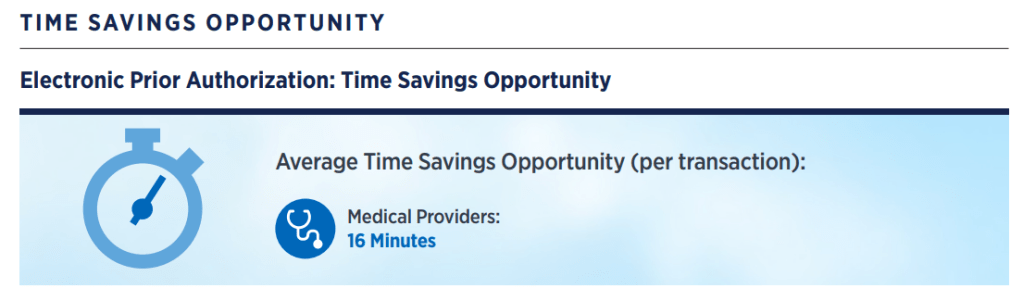
TIME (WASTED!)
Time Savings Opportunity — The time that providers could save by switching the remaining partially electronic and fully manual time to conduct a transaction to a fully electronic time.
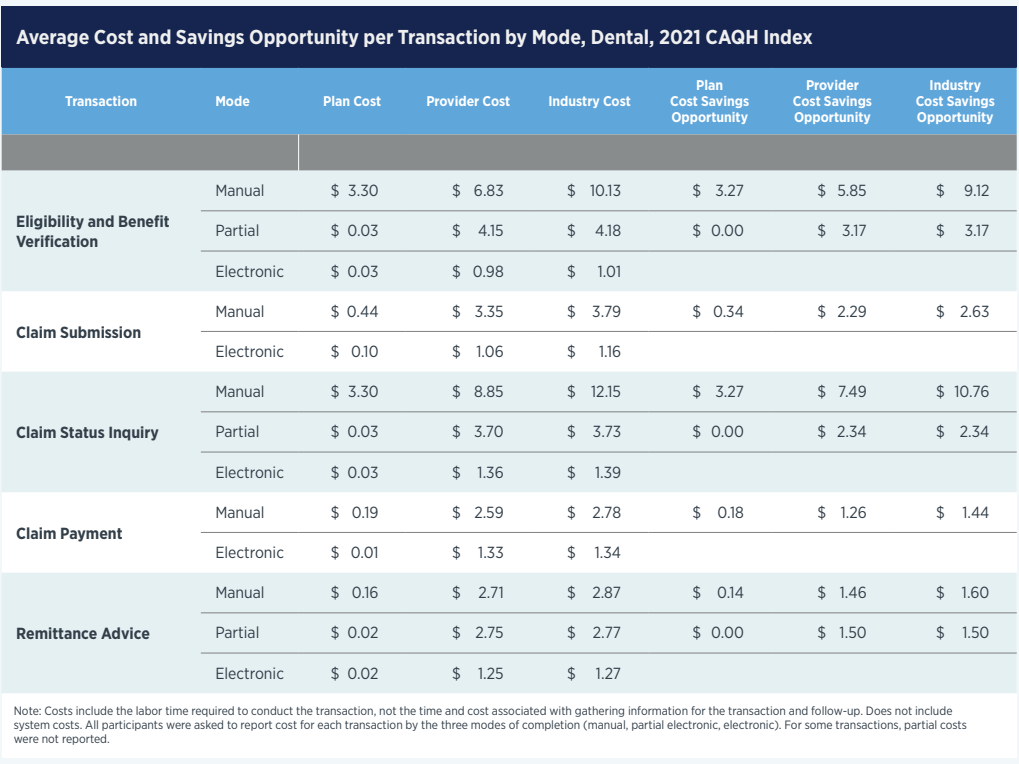
Average Cost and Savings Opportunity per Transaction by Mode, Dental, 2021 CAQH Index