The tool is easy to use and only requires a handful of questions about your institution, including enrollment size, approximate institutional drop-out rate, and approximate per student tuition rate. Based on this information, the calculator will give economic estimates for both your institution and students.
This tool will allow you to calculate the economic returns of services or programs that improve mental health in your student population.
You will be asked a handful of questions about your campus, including:
Enrollment size
Approximate institutional drop-out rate
Approximate per student tuition rate
Based on the information you provide, the calculator will give economic estimates for both your institution and students.
Your proposed services or programs could be focused on mental health treatment or could also seek to prevent mental health issues. They could be new or expanded offerings that your campus is considering, or they could be existing services.
The calculator’s estimates are based on research by the Healthy Minds Network. This research examined how depressive symptoms predict student persistence in college. The estimates, therefore, are most accurate for services and programs that specifically reduce depressive symptoms. The estimates may also extend to services and programs that address other mental health concerns, such as anxiety. The original research article with more details is available here as well as the Healthy Minds website.
Advanced financial and statistical support relating to Capitation Rates, Risk Adjustment Models, and Payment Methodologies.
Medicaid Actuarial Services
This post is useful for those seeking information on Medicaid actuarial services and related rates in Florida.
Outlines Medicaid actuarial services provided by the Bureau, including advanced financial and statistical support for Capitation Rates, Risk Adjustment Models, and Payment Methodologies.
Provides information on Managed Medical Assistance (MMA), Long-Term Care (LTC), and Dental Capitation Rates for various years.
Includes a link to a Special Needs Plan Revenue and Expense Schedule Statement Template Tool.
Unit Responsibilities include:
Support of Capitation Rate Development and Adjustment
Management of External Actuarial Service Contracts
Monitoring Medicaid Program Changes
Trend Analysis
Rate Impact Analysis
Medicaid Actuarial Services
This post is useful for those seeking information on Medicaid actuarial services and related rates in Florida.
Outlines Medicaid actuarial services provided by the Bureau, including advanced financial and statistical support for Capitation Rates, Risk Adjustment Models, and Payment Methodologies.
Provides information on Managed Medical Assistance (MMA), Long-Term Care (LTC), and Dental Capitation Rates for various years.
Includes a link to a Special Needs Plan Revenue and Expense Schedule Statement Template Tool.
For Institutional Reimbursement rates, please click here.
This dataset contains the total number of Medi-Cal Managed Care enrollees based on the reported month, plan type, county, and health plan.
This dataset contains the total number of Medi-Cal Managed Care enrollees based on the reported month, plan type, county, and health plan.
Medi-Cal Managed Care Enrollment Report
The Medi-Cal Managed Care Enrollment Report is a dataset that contains information about the number of people enrolled in Medi-Cal Managed Care plans based on reported month, plan type, county, and health plan. This report is an important tool for policymakers and researchers who want to better understand the state of healthcare in California.
The dataset provides valuable insights into the number of people enrolled in Medi-Cal Managed Care plans, which are designed to provide affordable healthcare to low-income Californians. By analyzing the data in the report, policymakers and researchers can identify trends in enrollment, plan type, and county-level differences in enrollment rates.
One important trend that the report highlights is the increasing popularity of Medi-Cal Managed Care plans. As of the latest reported month, the total number of people enrolled in these plans was higher than ever before, indicating that more Californians are taking advantage of these affordable healthcare options.
Another important trend is the differences in enrollment rates across different counties in California. The report shows that some counties have higher enrollment rates than others, indicating that there may be disparities in access to healthcare across the state.
Overall, the Medi-Cal Managed Care Enrollment Report is an essential resource for anyone interested in understanding the state of healthcare in California. By providing detailed information about enrollment in Medi-Cal Managed Care plans, this report can help policymakers and researchers identify areas where improvements can be made, and ensure that all Californians have access to affordable, high-quality healthcare.
The CAQH Index benchmarks adoption, volume, cost savings opportunities and spend for transactions along the administrative workflow. The following metrics help measure progress towards an automated workflow. By tracking progress, the industry can more easily identify barriers that may be delaying automation and administrative simplification and focus efforts on them.
2021 CAQH INDEX®
The CAQH Index benchmarks adoption, volume, cost savings opportunities and spend for transactions along the administrative workflow.
The CAQH Index benchmarks adoption, volume, cost savings opportunities and spend for transactions along the administrative workflow. The following metrics help measure progress towards an automated workflow. By tracking progress, the industry can more easily identify barriers that may be delaying automation and administrative simplification and focus efforts on them.
ADMINISTRATIVE WORKFLOW
While COVID-19 touched all healthcare professionals, the pandemic impacted the medical and dental administrative workflows differently.
The following touches on MEDICAL and DENTAL.
Utilization
Policies developed by federal and state entities to curb the spread of COVID-19 resulted in lower utilization for both industries as people delayed, or went without, medical care. In general, lower utilization led to lower transaction volumes. Smaller dental practices were hit particularly hard by lower utilization as many offices were forced to close for several months or close permanently.
Spend
Although electronic adoption and volume increased for both industries, the spend associated with conducting administrative transactions varied. While the dental industry saw a drop in spend, the medical industry experienced an increase in spend as it dealt with more complicated factors related to COVID-19
Automation
As remote work increased, many medical and dental staff became more reliant on the use of electronic transactions to conduct business. Staff no longer had access to resources used to conduct manual transactions. Because of this, both industries saw an increase in electronic adoption.
Telemedicine
For the medical industry, the loss in volume was counterbalanced by the increase in telemedicine. Telemedicine expanded access to care while reducing exposure to the virus for staff and patients. Health plans and providers worked together to understand and confirm new requirements and varying codes around telemedicine which often resulted in costly and timely phone calls and manual work. And while manual volume dropped, manual transactions became more expensive, increasing overall spend and the cost savings opportunity.
While manual volume dropped, manual transactions became more expensive, increasing overall spend and the cost savings opportunity.
While manual volume dropped, manual transactions became more expensive, increasing overall spend and the cost savings opportunity.
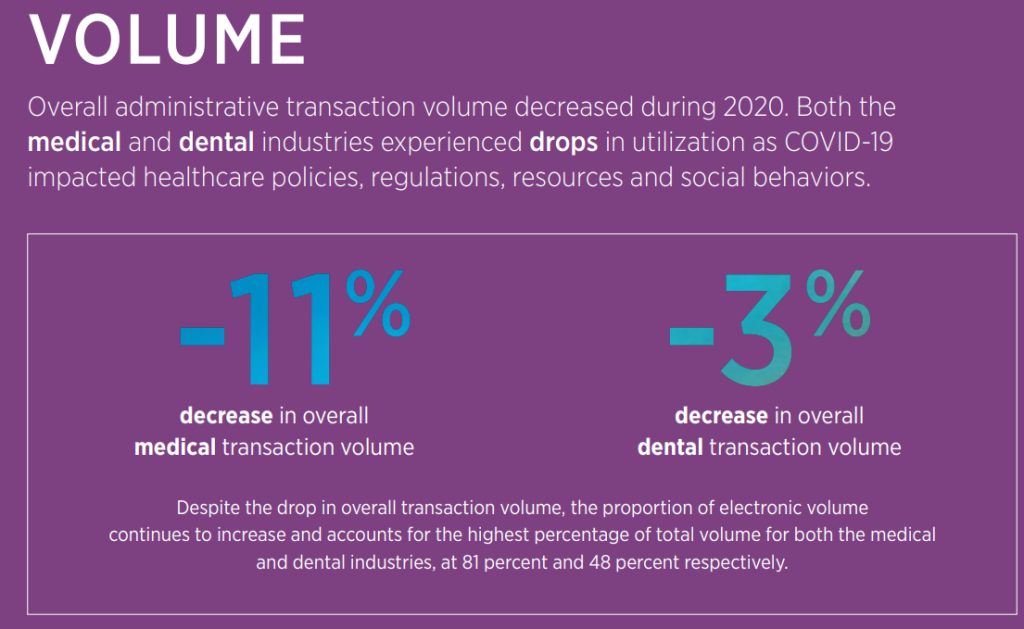
Overall administrative transaction volume decreased during 2020. Both the medical and dental industries experienced drops in utilization as COVID-19 impacted healthcare policies, regulations, resources and social behaviors.
SPEND
Despite the decrease in overall medical transaction volume and growth in electronic adoption, total annual medical spend increased (12%) as manual transactions required more intensive intervention from providers to ensure that newly implemented requirements and codes were executed correctly and that patient medical records were current and accurate. Conversely, dental spending decreased due to lower utilization often resulting in office closures.
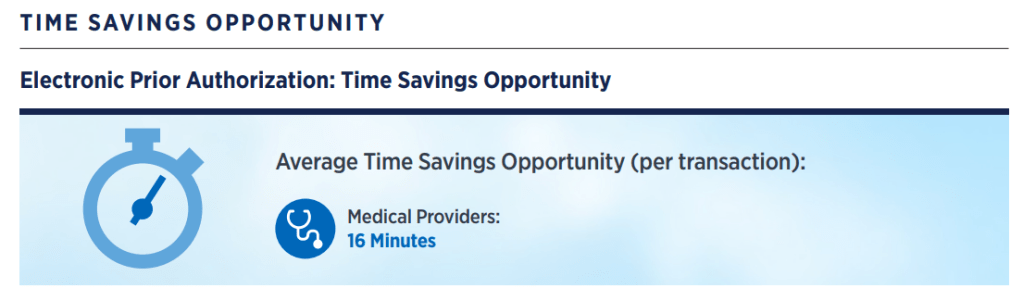
TIME (WASTED!)
Time Savings Opportunity — The time that providers could save by switching the remaining partially electronic and fully manual time to conduct a transaction to a fully electronic time.
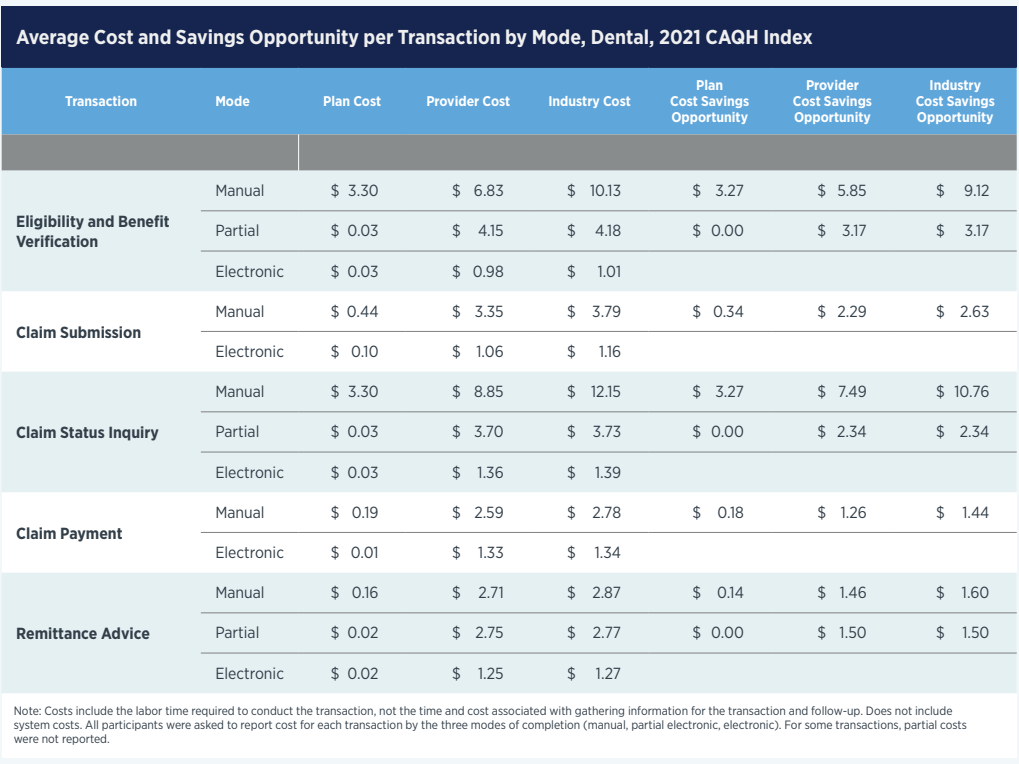
Average Cost and Savings Opportunity per Transaction by Mode, Dental, 2021 CAQH Index
Various reports from the State of California regarding the quality of care provided by Medi-Cal managed care health plans. Plan-specific evaluation reports are also prepared for each individual health plan reviewed.
The California Department of Health Care Services contracts with an external quality review organization to evaluate the care provided to Medi-Cal managed care beneficiaries in the areas of quality, access, and timeliness. Reports are available on the DHCS website, including member satisfaction surveys, encounter data validation study reports, managed care accountability sets, external quality review technical reports, plan-specific evaluation reports, health disparity reports, HEDIS® reports, MCP-specific performance evaluation reports, performance improvement project reports, and preventive services reports.
Outline
Introduction: Purpose of the DHCS external quality review organization
Available Reports:
Member Satisfaction Surveys
Encounter Data Validation Study Reports
Managed Care Accountability Sets/External Accountability Sets
External Quality Review Technical Reports and Plan-Specific Evaluation Reports
Health Disparity Reports
HEDIS® Reports
MCP-Specific Performance Evaluation Reports
Performance Improvement Project Reports
Preventive Services Report
Conclusion: Summary of available reports and their purpose.
In accordance with federal requirements, the California Department of Health Care Services (DHCS) contracts with an external quality review organization (EQRO) to conduct external quality reviews and evaluate the care provided to beneficiaries by Medi-Cal managed care health plans (MCPs) in the areas of quality, access, and timeliness. The EQRO presents these external quality review activities, results, and assessments in reports that help DHCS and Medi-Cal MCPs understand where to focus resources to further improve the quality of care.
External Quality Review Technical Reports and Plan-Specific Evaluation Reports
The EQRO annually prepares an independent external quality review technical report that analyzes and evaluates aggregated information on the health care services provided by Medi-Cal MCPs. As part of the external quality review technical report, the EQRO prepares a plan-specific evaluation report of each of MCP.
The Health Disparity Reports identify and understand health disparities affecting California’s Medi-Cal managed care members and are based on focused studies conducted annually by the EQRO. The reports analyze Managed Care Accountability Set (MCAS) measure results reported by Medi-Cal managed care plans (MCPs) for various demographic categories.
HEDIS® Reports
The Healthcare Effectiveness Data and Information Set (HEDIS®) Aggregate Report, also referred to as Performance Measurement Reports, provides performance rates of MCPs during a reporting year and trending using previous years’ data. The report also compares plan-specific and aggregated rates to national benchmarks.
MCP-Specific Performance Evaluation Reports
The MCP-Specific Performance Evaluation Reports are also referred to as Plan-Specific Performance Evaluation Reports.
The Birth Count Query System is a highly useful online tool provided by the Florida Department of Health. It offers a plethora of data on birth counts in Florida, and can be accessed easily through this link: https://www.flhealthcharts.gov/FLQUERY_New/Birth/Count.
This comprehensive tool is an excellent resource for researchers and analysts who are interested in delving deeper into birth trends in Florida. The system provides data that is updated regularly, offering a wealth of information on birth counts across different areas of the state, as well as various demographics. By using this system, researchers and analysts can gain valuable insights into the factors that affect birth rates in Florida, and can make informed decisions based on the data provided by the tool. Additionally, the system can also be used to identify areas where further research is needed, helping to drive innovation in the field of birth rate analysis.
The New Jersey Health Care Quality Act (HCQA), N.J.S.A. 26:2S-1 et seq. and rules establish certain rights AND responsibilities for health care providers that contract with carriers for business that is subject to the HCQA. Whether your contract with a carrier is subject to the terms of the HCQA depends upon whether the business for which you are to deliver health care services is subject to the HCQA.
The New Jersey Health Care Quality Act (HCQA), N.J.S.A. 26:2S-1 et seq. and rules establish certain rights AND responsibilities for health care providers that contract with carriers for business that is subject to the HCQA. Whether your contract with a carrier is subject to the terms of the HCQA depends upon whether the business for which you are to deliver health care services is subject to the HCQA.
The following rights apply to all health care providers:
The right to have your application to participate in the carrier’s network reviewed by a panel of health care providers, one of whom is knowledgeable in your scope of professional practice (but please note that this process and this committee may not be the same as the credentialing process or committee).
The right to submit the NJ Universal Physician Application or NJ Physician Recredentialing Application instead of carriers forms.
The right to receive a written decision regarding the application to participate within 90 days of providing the complete application.
The right to request and review the factors considered by the committee in reviewing applications.
The right to file complaints on your own behalf or on the behalf of your patient, with your patient’s consent, without fear of retaliation, and to have those complaints resolved.
The right to communicate openly with patients about all diagnostic testing and treatment options.
The right to act as an advocate for your patient in seeking appropriate, medically necessary health services.
The right to speak with the doctor who, acting on behalf of the carrier, disapproves or limits approval of a request for covered services, and receive a written statement denying the approval upon request.
The right to file with a carrier an internal Stage 1 and Stage 2 appeal of a disapproval or limited approval of covered services on behalf of your patient, with your patient’s specific consent.
The right to obtain a written decision at the conclusion of each stage of the internal appeal process explaining why the carrier’s prior decision is being upheld (if that is the case), and explaining how to proceed to the next level of appeal.
The right to pursue an external appeal through the Independent Health Care Appeals Program (IHCAP) on behalf of your patient, with the patient’s consent, and obtain a written decision from the Independent Health Care Appeals Program upon the conclusion of the appeal review process.
The right to receive a periodic accounting of withhold amounts.
The right to provide input in the clinical criteria and protocols adopted by the carrier, pursuant to a system for the provision of such input established by the carrier.
The right to appeal claims payment issues within 90 days following a claims determination, and then take matters of $1,000 or more to the New Jersey Program for Independent Claims Payment Arbitration (PICPA).
The right to aggregate claims to attain the $1,000 PICPA threshold.
The following additional rights apply to health care professionals:
The right to at least 90-days prior written notice of termination of the contract, and the right to request a hearing, if the termination is to occur on other than the renewal or anniversary date of the contract, unless the termination is based on a belief that you have committed a fraud, breached the terms of the contract, or are an imminent danger to a patient or the public health, safety and welfare.
The right to request a written reason for the termination, if one is not provided with the notice of termination.
The right to request a hearing within 10 business days of receipt of the notice of termination, and to have the hearing held within 30 days of the request for the hearing.
The right to have the hearing held before a panel of at least three people, one of whom is in the same or a substantially similar discipline and specialty as you, and to be present at the hearing with representation.
The right to receive in writing the decision of the panel within 30 days following the close of the hearing (unless the panel requests an extension). The decision must specify the reasons for the panel’s decision. If the panel recommends conditional reinstatement, the decision must include any conditions and time periods for conditional reinstatement, and the consequences for failing to meet the conditions.
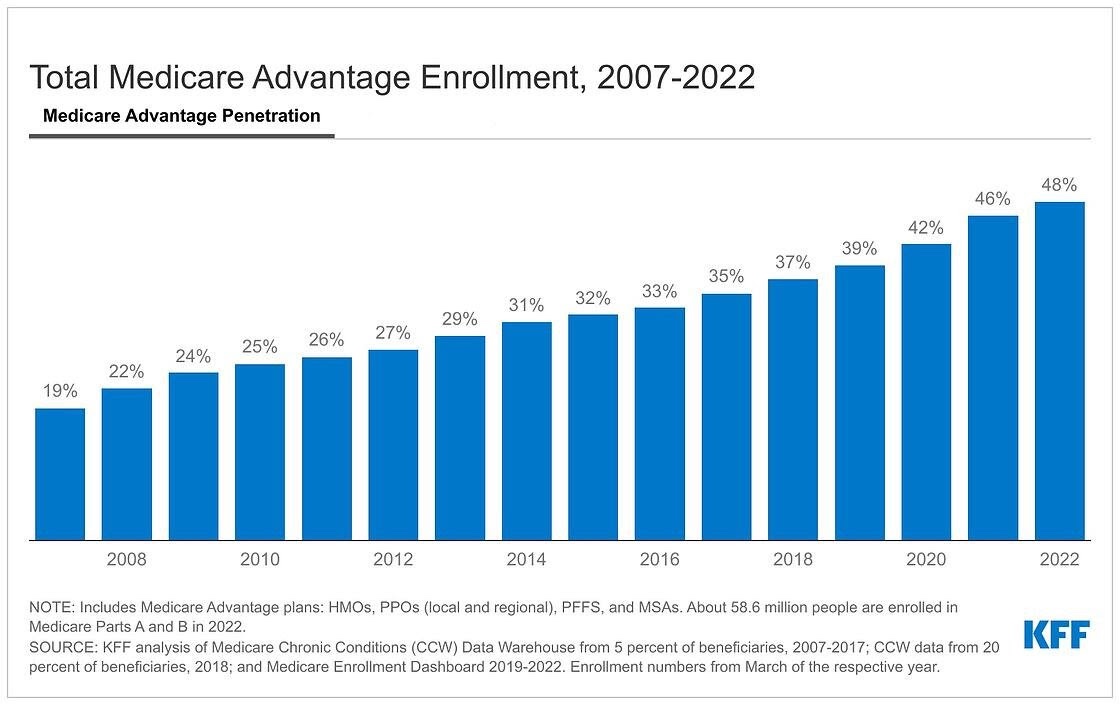
As Medicare Advantage continues to grow, a gradual but significant reshaping of the Medicare program is taking place.
A new KFF analysis finds that nearly half of eligible Medicare beneficiaries – 28.4 million out of 58.6 million Medicare beneficiaries overall – are now enrolled in Medicare Advantage plans. That represents a more than doubling of the share of the eligible Medicare population enrolled in such plans from 2007 to 2022 (19% to 48%). Enrollment is projected to cross the 50 percent threshold as soon as next year, making Medicare Advantage the predominant way that Medicare beneficiaries with Parts A and B get their coverage and care.