Understanding State-Level Variation in Supplemental Maternity Kick Payments in Medicaid Managed Care
Introduction
Today, we’re exploring an intriguing study on the state-level variation in supplemental maternity kick payments in Medicaid managed care. This study, conducted by Samantha G. Auty, Jamie R. Daw, and Jacob Wallace, provides valuable insights into how these payments impact delivery costs and care quality.
Post Introduction
In this post, we’ll break down the key findings of the study, understand the implications of kick payments on Medicaid managed care, and discuss how these variations can affect maternal health outcomes across different states. Let’s get started by understanding the basics of Medicaid managed care and why kick payments are essential.
Detailed Story
What is Medicaid Managed Care?
Medicaid managed care (MMC) involves states contracting with private health insurers to provide Medicaid coverage. This model covers about 70% of pregnant Medicaid enrollees and finances approximately 41% of all births in the United States. Under MMC, insurers receive per-member-per-month capitated payments to cover a defined set of benefits. However, covering pregnant individuals poses a higher financial risk due to their increased healthcare needs, which often leads to states implementing one-time “kick payments” to MMC plans triggered by delivery events.
The Role and Variation of Kick Payments
Kick payments are designed to offset the higher costs associated with childbirth. The rates and use of these payments can significantly influence whether MMC plans are incentivized to attract or avoid pregnant enrollees. This study aimed to assess the prevalence and magnitude of these kick payments across different states and how they align with actual delivery costs.
Research Methodology
The researchers conducted a cross-sectional study, abstracting data from state documents and MMC contracts published between 2018 and 2020. They gathered information on whether states used kick payments, the services covered by these payments, and the specific rates.
Additionally, they compared these rates with average state Medicaid fee-for-service (FFS) payments for delivery hospitalizations in 2020 and the Medicaid-Medicare fee index.
Key Findings
The study revealed that out of the 38 states and the District of Columbia using comprehensive MMC, 33 states used maternity kick payments. These payments varied significantly, ranging from $2,838 in New Hampshire to $14,493 in Maryland. Interestingly, the variation in kick payment rates did not correlate with the Medicaid payments to physicians or the actual delivery costs, indicating that in some states, kick payments might exceed delivery costs, while in others, they fall short.
These payments varied significantly, ranging from $2,838 in New Hampshire to $14,493 in Maryland.
Tweet
Expert Insights
To further explore the implications of these findings, let’s delve into some expert insights.
Potential Implications of Low Kick Payment Rates
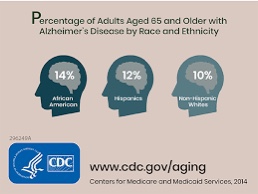
When kick payment rates are set too low, MMC plans might attempt to limit services for pregnant enrollees or restrict access to maternity care providers. This can lead to disparities in care quality and access, particularly affecting Black and Indigenous women, who are disproportionately enrolled in Medicaid and face higher risks of maternal mortality and morbidity.
The Need for Aligned Incentives
Aligning kick payment rates with actual delivery costs and care quality is crucial. States need to design Medicaid payment policies that support maternal health and promote health equity. This requires continuous research to understand the effects of these payments on care access, quality, and outcomes.
In-Depth Analysis
The Study’s Limitations
While the study provides valuable insights, it has some limitations. It could not directly associate kick payment rates with MMC plan behavior or maternal health outcomes. Additionally, the comparison was made with Medicaid FFS payments rather than the prices MMC plans paid for delivery services, which were unavailable.
The Path Forward
Further research is essential to evaluate the impact of kick payments on maternal care access and outcomes. Policymakers need comprehensive data to design effective Medicaid payment strategies that ensure equitable and high-quality maternal care.
Practical Tips
For state policymakers and healthcare administrators:
- Regular Review of Kick Payment Rates: Ensure that kick payment rates are regularly reviewed and adjusted to reflect actual delivery costs and care quality needs.
- Focus on Health Equity: Design payment policies that address disparities in maternal health outcomes, particularly for vulnerable populations.
- Data-Driven Decision Making: Use comprehensive data to evaluate the impact of payment policies on maternal care access and outcomes.
FAQ Section
Q1: What are Medicaid managed care kick payments? A: Kick payments are one-time payments made to Medicaid managed care plans to offset the higher costs associated with childbirth.
Q2: Why do kick payment rates vary between states? A: The variation can be due to different state policies, healthcare costs, and the structure of Medicaid managed care contracts.
Q3: How can low kick payment rates affect maternity care? A: Low rates can lead to MMC plans limiting services for pregnant enrollees or restricting access to maternity care providers, affecting care quality and access.
Q4: What can states do to improve kick payment policies? A: States should regularly review and adjust kick payment rates, focus on health equity, and use data-driven approaches to design effective payment policies.
Source
State-Level Variation in Supplemental Maternity Kick Payments in Medicaid Managed Care